Carmen P. DiGiovine1 PhD ATP/SMS RET; Mark I. Bresler2, MBME, PE, ATP;
Patricia A. Bahr3, MSE, RET
1The Ohio State University Wexner Medical Center; 2Woods Services;
3Gillette Children's Specialty Healthcare
Abstract
As the fields of assistive technology and rehabilitation technology have advanced, so has the role of the rehabilitation engineer. The RESNA-PSG for Rehabilitation Engineers and Technologists (RE&T) commissioned an ad-hoc committee to generate a white paper defining the roles and responsibilities of Rehabilitation Engineers in practice. This is the first product of the ad-hoc committee. The purpose of this article is to provide an overview of Rehabilitation Engineering and discuss the lessons learned as the field moves forward. As the field of rehabilitation engineering advances from the 1950’s until today, numerous opportunities exist in terms of professionalization, education and training, research and development, and credentialing. The role of the rehabilitation engineer has changed significantly over the past 6o years, but the one thing that remains the same is the application of engineering practices to improve the quality of life for individuals with disabilities.
Introduction
As assistive technology (AT) and universal design allows more people with disabilities to interact, participate, and thrive in our world, the role of the Rehabilitation Engineer (RE) has evolved. Initially, REs focused on developing custom devices in clinical settings. As more AT devices have transitioned from the realm of custom devices to the realm of commercially available devices (Figure 1), the role of REs have changed. REs now have a greater role in research and product development activities. For adult populations, rehabilitation engineers continue to make custom and modified AT in the vocational setting, and integrate numerous AT devices for a turnkey solution. For children, rehabilitation engineers consult in primary and secondary educational settings, allowing children to reach their full potential within the school.
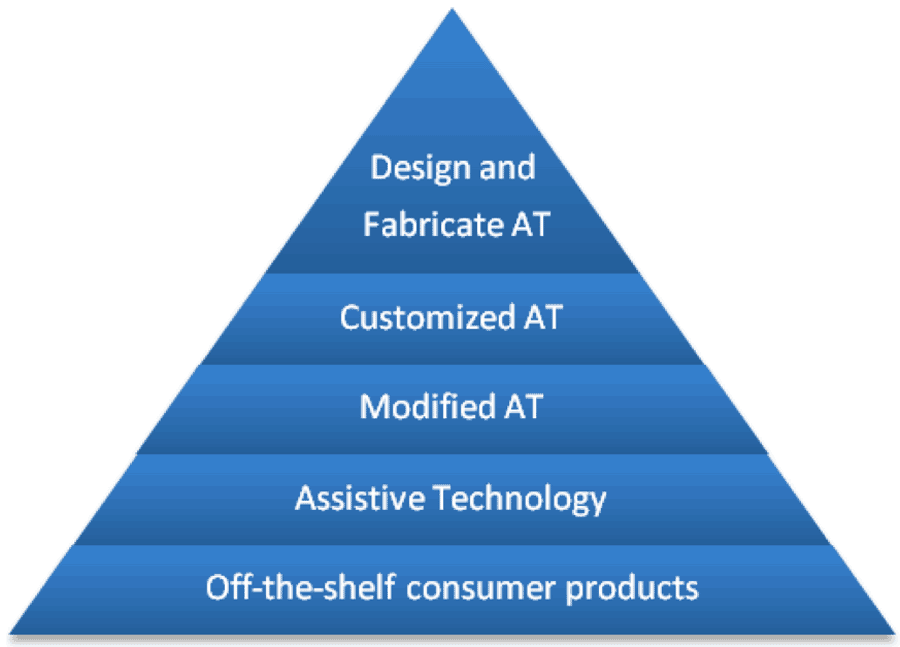 Figure 1. The continuum of assistive technology.
Figure 1. The continuum of assistive technology.As the fields of assistive technology and rehabilitation technology have advanced, so has the role of the rehabilitation engineer. In order to address this change, the Rehabilitation Engineering and Assistive Technology Society of America (RESNA), Rehabilitation Engineer and Technologist (RE&T) Professional Specialty Group (PSG) commissioned an ad-hoc committee to generate a white paper that defines the current roles and responsibilities of Rehabilitation Engineers in practice. This is the first product of the ad-hoc committee. The purpose of this article is to provide an overview of Rehabilitation Engineering and discusses the lessons learned as the field moves forward.
Background
Definition
Rehabilitation Engineering in the United States and Canada developed as a result of an unmet need to support individuals with disabilities throughout the latter half of the 20th century, as is described below. As a result, the term rehabilitation engineer and rehabilitation engineering began to appear in the literature. One of the earliest definitions of rehabilitation engineering is “the application of engineering and other sciences in combination with medicine to improve the quality of life of disabled persons.” (Reswick, 1980) Reswick goes on to describe the characteristics of Rehabilitation Engineers.
- The rehabilitation engineer must, first of all, be a competent professional in a specific field of specialization (e.g., mechanical, electrical, systems, chemical, materials engineering, O/P).
- The RE should have natural propensities for working with health professionals as a member of a patient-care team and to share responsibility with other team members.
- The RE practices a profession that assumes the highest ethical norms of both the engineering and health professions
- The RE often must relate closely with the commercialization of devices
- Above all, the rehabilitation engineer is patient- or client-oriented.(Reswick, 1980)
Over 30 years have elapsed, yet this definition and description of rehabilitation engineering still accurately describe the occupation. Though the field has evolved, and numerous definitions for rehabilitation engineering have been described in the literature(Hobson & Trefler, 2000; Hobson, 1977; Kondraske, 2000; Potvin, Mercadante, & Cook, 1980; Reswick, 1983), one of the simplest and most straight-forward definitions, which builds off of Reswick’s definition, is provided by the IEEE Engineering in Medicine and Biology Society. The definition simply states: “Rehabilitation Engineering is the application of science and technology to improve the quality of life for people with disabilities.”(IEEE-EMB, 2003) The definition is eloquent in that it first describes engineering as an activity, and then defines the population for which the activity is applied(Voland, 2004). This clearly identifies the uniqueness of engineers, as opposed to inventors or scientists, and the uniqueness of rehabilitation engineers.
United States’ History
Rehabilitation engineering in America owes its birth to the federal agencies that fostered its development after they had been so successful in supporting programs of research, education, and development in limb prosthetics and orthotics (initially for veterans) during the period from 1945 to 1970.
The polio epidemic in the early 1950s created a second wave of political and social will to do something for individuals with disabilities.
Engineers and orthotists were integrated into clinical teams in notable locations such as Rancho Los Amigos Hospital in Downey, CA and Baylor University in Houston. These programs again produced technical innovations for persons with reduced limb and upper body function due to neuromuscular disease and resulting dysfunction. At Rancho, Dr. Vern Nickel, a dynamic orthopedic surgeon, lead the team of James Allen, Dr. Vert Mooney, and treatment therapists that produced the early powered upper extremity orthosis, termed the “Rancho Golden Arm,” as well as many other simpler orthotic innovations. These early trials also demonstrated the limits of people’s gadget tolerance to encumbering technology. This was important knowledge; widespread acceptance would require more elegant solutions such as that promised by functional electrical stimulation. These and other early engineering achievements at Rancho laid the foundation for the initiation of the first Rehabilitation Engineering Center (REC) on functional electrical stimulation at Rancho in 1971, directed by James Reswick(Hobson, 2002). In the late 1960s, A. Bennett Wilson, Jr., Director of CPRD; Joseph Traub of the Rehabilitation Services Administration; Anthony Staros of VA; and others (engineers Colin McLaurin and James Reswick, for example) promoted the concept of Rehabilitation Engineering Research Centers as an enlargement of the very successful prosthetics programs. McLaurin and Reswick were rehabilitation engineering role models for me and for many entering the field. All of these individuals are considered pioneers of the rehabilitation engineering movement in the United States—perhaps A. Bennett Wilson, Jr., most of all. Nevertheless, the program could not have been consummated without the background support (political and otherwise) of surgeons and physicians such as William Berenberg of Boston, Clinton Compere of Chicago, Vernon Nickel of Los Angeles, George T. Aitken of Grand Rapids, William Spencer of Houston, Richard Herman of Philadelphia, and many others. It was a team effort.(Childress, 2002)
Clients
Based on the framework established by these pioneers, Rehabilitation Engineering has also advanced through the years to address the needs presented by changing disability demographics. From the development of the prosthetic field as a result of WWII, the polio epidemics of the 1950s and before, REs have been involved in making technology that improved the lives of people with disabilities.
Medical advances have changed the face of disability too. Smaller babies survive; some with disabilities. More individuals survive from injuries as a result of catastrophic events than ever before. These events range from car accidents and violent crimes within the United States to combat injuries acquired by soldiers on the battle field. Also, there is an aging population that seeks to remain in the home setting as long as possible. All of these individuals need assistive technology, and rehabilitation technology. Rehabilitation engineering, given it’s focus on the unique needs of individuals with disabilities, and the ability to work in a multi-disciplinary setting, is poised to develop and integrate the technology to improve the quality of life of individuals with disabilities, today and in the future.
Work Setting
While rehabilitation engineering and assistive technology on the surface are specialties, a closer look shows many practitioners operating in diverse sub specialties. As the research fundamentals of rehabilitation engineering were being established, facilities and workgroups within diverse rehabilitation facilities were providing service delivery to a wide range of clients. Some of this diversity was captured in a 1984 RESNA conference paper(Bresler, 1984) which provided snapshots of seven practitioners.
Work settings included hospitals, Veterans Administration hospitals, school districts, state vocational rehabilitation, and rehabilitation facilities. Job tasks included seating and positioning, home modifications including bathroom modifications and wheelchair ramps, and job site modification.
In 1991, Trachtman noted that Rehabilitation Engineers worked in service delivery, research and development, management and administration, policy and planning, education and training, and sales and marketing(Trachtman, 1991). Those providing service delivery worked primarily in hospitals, universities, education or vocation agencies, and private practice as consultants. Those working in research and development worked primarily in universities and hospitals.
By 2007, Downey noted that even though more assistive technology was available, there was still need for rehabilitation engineers(Downey, 2007). This was due to the small market for new products, and the continued need for custom modifications and product development.
EDUCATION AND TRAINING
As the field of Rehabilitation Engineering advanced through the late 1970s and 1980s, most notably with the start of the Rehabilitation Engineering Society of North America (RESNA) in 1979, so did opportunities for education and training. A call for education and training in rehabilitation science and engineering was described in 1997 in “Enabling America”(Brandt & Pope, 1997). In this book, the authors make four recommendations, of which one is to increased doctoral and postdoctoral education “…to help encourage the development of the field and respond to the expanding research needs.” Therefore, the education and training opportunities have primarily focused on activities surrounding the Rehabilitation Engineering Research Centers, which continues today.
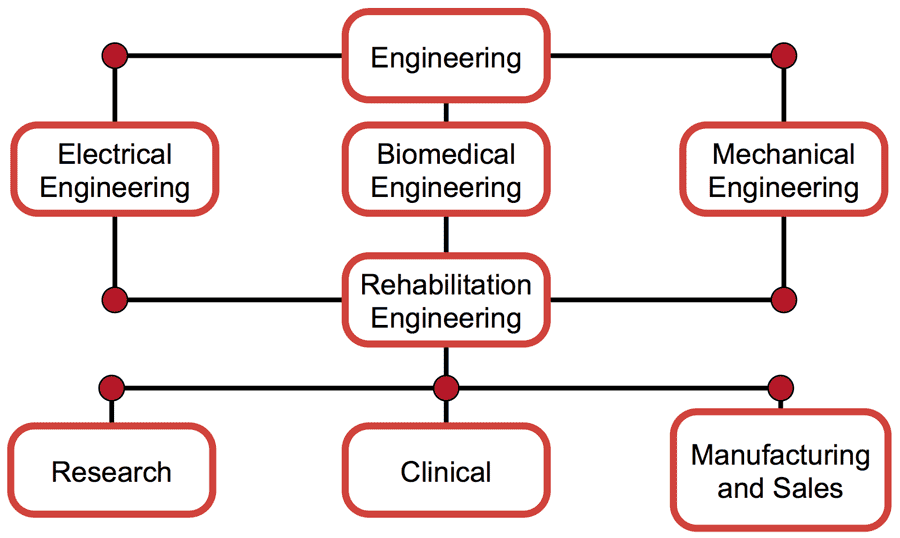 Figure 2. Example engineering educational programs that feed into RE, and the associated areas of employment.
Figure 2. Example engineering educational programs that feed into RE, and the associated areas of employment.As another avenue for education and training, many engineering capstone design programs, which take place during the senior year of the bachelor degree programs, focus on issues related to individuals with disabilities. Though, traditional programs in rehabilitation engineering do not currently exist at the undergraduate level, the principles of rehabilitation engineering are incorporated into the program, most notably in the departments of biomedical engineering, electrical engineering, and mechanical engineering (Figure 2). At the graduate level, rehabilitation engineering is embedded in numerous research activities. Therefore, even though formal educational programs in rehabilitation engineering do not currently exist, numerous opportunities for specializing in rehabilitation engineering are currently available within multiple engineering disciplines. In the future, these opportunities may turn into dedicated training programs within the Engineering and Rehabilitation Sciences curricula.
PROFESSIONAL ORGANIZATIONS
Rehabilitation Engineering has been a component of numerous professional organizations throughout the years. Traditionally, rehabilitation engineering has had a theme in the IEEE-EMB conference and the BMES conference. However, no professional organization has done as much to support rehabilitation engineering as RESNA. The multi-disciplinary nature of RESNA makes it the ideal professional organization to support professionals in the field of rehabilitation engineering. Though other professional organizations, such as IEEE-EMB and BMES, support engineering activities, they do not provide opportunities to fully integrate technology within the multi-disciplinary context of rehabilitation engineering.
In the future, the professional organizations that support rehabilitation engineering activities need to work together to support the professionals they represent. Given the significant changes that are occurring within the technology fields, and the changes that are occurring within state and federal policy, the organizations need to provide a single voice for increasing the recognition of rehabilitation engineering.
CREDENTIALS
Credentialing of rehabilitation engineers has been a key discussion within the field of rehabilitation engineering. As noted in “RESNA's Credentialing Program: A History and Current Status Report”, RESNA investigated the possibility of creating a certification for rehabilitation engineers under the auspices of a quality assurance program starting in the late 1980’s and early 1990’s. In 1994, the Professional Standards Board in Assistive Technology and Rehabilitation Engineering was established by the RESNA Board of Directors. The original thought was to have a Rehabilitation Engineering certification that required a PE license, the ATP Certification, and a demonstrated competency in rehabilitation engineering(Minkel, 1996). This transitioned into the Rehabilitation Engineering Technologist certification, which required the ATP certification, the RET certification exam, and demonstrated experience in rehabilitation engineering. The change in requirements was predicated on the need to include a broader range of professionals that work in the fields of rehabilitation engineering and rehabilitation science. This lead to the first RET certification exam which was administered in 2002. Over the course of the certification, 48 individuals acquired the certification. Given the low numbers, the certification was placed on hold in 2010 in order to address the current rigor of the certification and develop a plan for future credentialing of rehabilitation engineers. An ad-hoc committee on Rehabilitation Engineering certification was convened in 2013 by the RESNA Board of Directors with representation from the BOD, the Professional Specialty Group, and the PSB to directly address the future of a rehabilitation engineering credential.
CONCLUSIONS
Since the Journal of Rehabilitation Research and Development, November/December 2002, Supplement from which much of the history in this proceeding was drawn(Childress, 2002; Hobson, 2002), some things have changed but others have stayed the same. As commercially available assistive technology and universal design allows more people with disabilities to interact, participate, and thrive in our world, the role of the Rehabilitation Engineer has evolved. More rehabilitation engineers now work in research and product development with fewer in medical clinic settings. For elderly, rehabilitation engineers allow individuals to stay in their home, for adults, they continue to make custom vocational adaptations, and for children, rehabilitation engineers consult in medical clinics, and primary and secondary educational settings.
References
Brandt, E. N., & Pope, A. M. (Eds.). (1997). Education and Training in Rehabilitation Science and Engineering. In Enabling America: Assessing the Role of Rehabilitation Science and Engineering (pp. 217–243). Washington, DC: National Academy Press.
Bresler, M. I. (1984). Workload of Service Delivery Rehabilitation Engineers. In Proceedings of the 2nd international conference on rehabilitation engineering (pp. 311–313).
Childress, D. S. (2002). Development of rehabilitation engineering of the years: As I see it. J Rehabil Res Dev, 39(6, supplement), 1–10.
Downey, G. (2007). What is a Rehab Engineer and Why Do you Need One? Rehab Pro, 15(1), 33–36.
Hobson, D. A. (1977). Rehabilitation engineering--a developing specialty. Prosthet Orthot Int, 1(1), 56–60.
Hobson, D. A. (2002). Reflections on rehabilitation engineering history: Are there lessons to be learned? J Rehabil Res Dev, 39(6, supplement), 17–22.
Hobson, D. A., & Trefler, E. (2000). Rehabilitation Engineering Technologies: Principles of Application. In J. D. Bronzino (Ed.), The Biomedical Engineering Handbook (Vols. 1-Book, 1-Section, Vol. 2, pp. 146–1 – 146–9). Boca Raton, FL: CRC Press LLC.
IEEE-EMB. (2003). Designing a Career in Biomedical Engineering (p. 20). Piscataway, NJ: IEEE Engineering in Medicine and Biology. Retrieved from http://www.embs.org/docs/careerguide.pdf
Kondraske, G. V. (2000). Measurement Tools and Processes in Rehabilitation Engineering. In J. D. Bronzino (Ed.), The Biomedical Engineering Handbook (Vols. 1-Book, 1-Section, Vol. 2, pp. 145–1 – 145–16). Boca Raton, FL: CRC Press LLC.
Minkel, J. L. (1996). RESNA’s Credentialing Program: A History and Current Status Report (p. 12). Arlin: Rehabilitation Engineering and Assistive Technology Society of North America.
Potvin, A. R., Mercadante, T. C., & Cook, A. M. (1980). Skill requirements for the rehabilitation engineer: results of a survey. IEEE Trans Biomed Eng, 27(5), 283–8.
Reswick, J. B. (1980). Rehabilitation engineering. Annu Rev Rehabil, 1, 55–79.
Reswick, J. B. (1983). Technology--an unfulfilled promise for the handicapped. Medical Progress through Technology, 9(4), 209–215.
Trachtman, L. H. (1991, June). Who is a Rehabilitation Engineeer? Team Rehab Report, 46–48.
Voland, G. (2004). Engineering by design (2nd ed.). Upper Saddle River, N.J.: Pearson/Prentice Hall.
ACKNOWLEDGEMENTS
The authors wish to acknowledge contributions from additional members of the RESNA ad-hoc committee: Patti Barrett, Brian Burkhardt, Bill Calvin, Yaghoub Dabiri, Steven Dahling, Peter Dollard, Meghan Donahue, Joe Klaesner, Rick Nelson, Raj Pagadala, David Savage, Rich Schein, Jerry Weisman, and Joann Willis.
Audio Version PDF Version